
Introduction (TL;DR): Medical coding demands pinpoint accuracy, but what happens when a physician provides a highly detailed diagnosis, yet no specific ICD-10 code perfectly matches it? Are you forced to use a vague, unspecified code, potentially misrepresenting the patient's condition and impacting billing? This article unravels the mystery of "Not Elsewhere Classified" (NEC) codes, guiding you through their precise application, distinguishing them from the often-confused "Not Otherwise Specified" (NOS) codes, and demonstrating why mastering NEC is non-negotiable for compliant, accurate, and effective medical coding.
What is NEC? Understanding the NEC Code in Medical Coding
Medical coding is all about precision. The codes used in healthcare documentation impact everything from patient care to insurance reimbursement. But what happens when a provider documents a diagnosis with great detail, and yet no specific ICD-10 code exists to match it? That's where the NEC code comes in.
Short for "Not Elsewhere Classified," this coding convention plays a key role in capturing unique diagnoses that don't fit neatly into the existing classification system. It also highlights the importance of standardized codes for accurate recordkeeping across healthcare settings.
Understanding when and how to use the NEC code is essential for ensuring accuracy and compliance in medical records and the broader medical billing process.
What Does NEC Mean in Medical Coding?
In the ICD-10-CM system, the NEC code stands for "Not Elsewhere Classified." This designation is used when a provider documents a diagnosis in specific detail, but there is no individual code available in the classification system to capture that exact diagnosis. It's a coding convention designed to ensure that a specific and well-documented medical condition can still be coded, even if the system has not yet created a dedicated entry for it.
NEC Reflects Specific Documentation
Many people mistakenly think NEC codes are used when documentation is unclear. In reality, NEC codes are used when the provider's documentation is detailed and specific, but no exact ICD-10-CM code exists to match it. The provider has thoroughly described the condition, but ICD-10 does not currently offer a more accurate code to represent that diagnosis. This is why medical coders must stay informed and understand the structure of standardized coding systems.
For example, if a provider records a rare or newly identified condition and there is no exact code listed under any of the relevant ICD-10 categories, a coder may need to use an NEC code to best reflect the specificity provided.
Understanding when and why to use an NEC code helps coders protect the accuracy of medical records, support compliant billing practices, and ensure that providers' detailed documentation is properly reflected in the coding process.
When No Exact Code Exists
ICD-10-CM is designed to be a detailed and comprehensive system. However, it's not possible for it to account for every emerging or rare diagnosis. In these cases, coders rely on NEC to ensure the record still accurately represents the provider's intent and the patient's condition.
NEC codes serve as a bridge between what is documented and what the coding system currently allows. They are particularly important in areas like documenting medical procedures or evolving healthcare services, where new innovations may not yet have dedicated classifications.
For coders, this means regularly reviewing ICD-10-CM conventions and staying up to date with any updates that might add more precise codes in the future.
Specificity Is Still the Goal
The ultimate objective of using the NEC code is to maintain accuracy while still coding to the highest level of specificity. ICD-10 encourages coders to assign the most detailed and appropriate code possible based on the available documentation. NEC supports that principle when the system itself is the limiting factor. This is important across all types of medical services, from outpatient visits to ambulance services, ensuring that even emerging conditions are accurately tracked.
In all cases, providers and coders should work together to ensure documentation is clear and complete. This not only improves the selection of codes like NEC but also supports billing accuracy, compliance, and quality patient care.
NEC vs. NOS (Unspecified): Understanding the Difference
In medical coding, understanding the difference between NEC and NOS is essential for selecting the most accurate code. While both terms are part of the ICD-10-CM coding system, they are used in very different circumstances. Confusing them can lead to inaccurate documentation and potential compliance issues. Medical coders must be especially cautious to distinguish between these two when processing complex cases like ambulance services or specialized medical procedures.
What Does NOS Mean in Medical Coding?
NOS stands for "Not Otherwise Specified." It is also commonly referred to as "unspecified" in code descriptions. This designation is used when the documentation from the provider is too vague or general to assign a more specific code.
In other words, the diagnosis may fall into a broad category, but additional detail is missing. That detail might be unavailable because the provider hasn't yet determined it or simply didn't document it clearly.
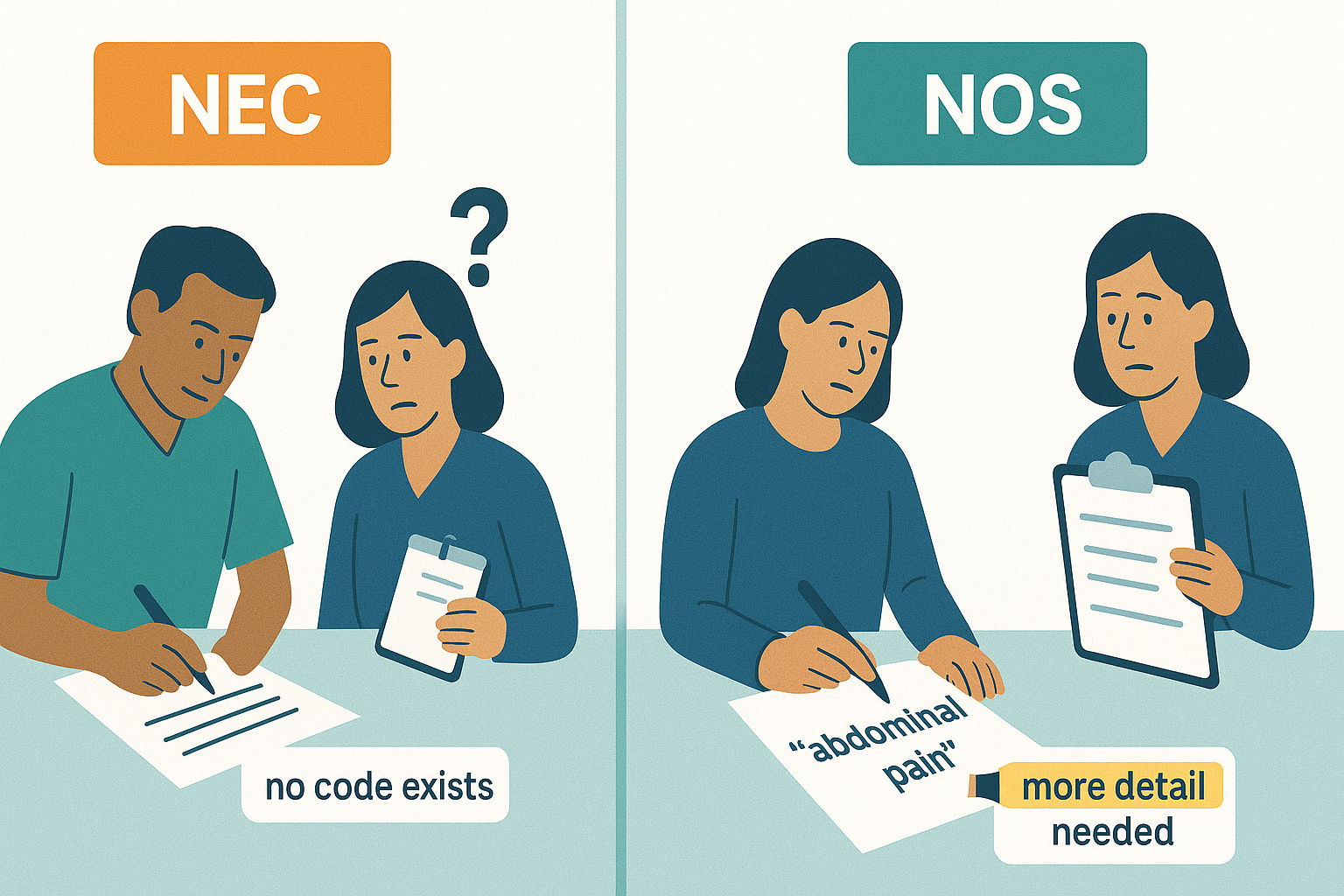
For example, a diagnosis of "abdominal pain" without additional information about the location or cause would lead to the use of an unspecified code. Similarly, "pneumonia, unspecified" might be used if the type or source of the pneumonia was not documented.
Key Differences Between NEC and NOS
Although they may seem similar at a glance, NEC and NOS serve different purposes and reflect different documentation scenarios:
●
NEC is used when the provider offers specific, detailed documentation, but no unique ICD-10 code exists to match
that exact diagnosis.
● NOS is used when the provider's documentation is too general or lacks sufficient detail, making it impossible to assign a more precise code.
These differences impact how coders interpret documentation and select the appropriate diagnosis codes. NEC reflects limitations in the coding system, while NOS reflects limitations in the documentation itself.
Common Misunderstandings About NEC and NOS
A common mistake is assuming that NEC and NOS are interchangeable. However, using NOS when NEC is appropriate, or vice versa, can lead to claim rejections or inaccurate records. Coders should carefully read both the provider's documentation and the code descriptions to determine whether the lack of specificity lies in the record or in the classification system.
Additionally, understanding the correct use of NOS and NEC is essential when dealing with temporary codes assigned for new medical procedures or Medicaid Services reporting requirements.
Encouraging More Precise Documentation
One of the best ways to avoid unnecessary use of NOS codes is through improved documentation. Providers should be encouraged to include as much clinical detail as possible. For coders, this means collaborating with providers and offering feedback when documentation lacks the specificity needed to assign accurate codes.
Not only does this support compliance and billing accuracy, but it also contributes to better patient care and more meaningful data for population health and research purposes.
For more tips on working with diagnosis
codes and staying compliant, explore our resources on ICD-10 coding best practices.
When and How to Use NEC Codes Correctly
Accurate use of the NEC code is essential for ensuring that medical records reflect the provider's intent and the patient's actual condition.
According to the official ICD-10-CM coding guidelines, NEC codes should be used when the documentation is specific and thorough, but the ICD-10 system does not include an exact match for the diagnosis provided. In these cases, NEC offers a way to code the diagnosis without compromising on detail. This attention to detail benefits healthcare providers and strengthens the consistency of data across standard code systems.
Understanding when to use NEC is only part of the equation. Coders must also follow official guidelines carefully to ensure the code is applied correctly and to avoid potential compliance risks. Let's take a closer look at what the ICD-10-CM guidelines say about NEC coding.
Follow the ICD-10-CM Guidelines
The ICD-10-CM guidelines instruct coders to select the code that best matches the provider's documentation. When a detailed diagnosis is documented but no specific ICD-10-CM code exists for it, the NEC code should be used. This approach ensures that the diagnosis is still captured accurately, maintains the integrity of the medical record, and respects the provider's clinical detail within the coding system. Staying current with ICD-10-CM changes is critical for medical coders, especially when Medicaid Services policies are updated or when new procedural codes are introduced into the classification system.
Using NEC improperly, especially when a more accurate code does exist, can lead to denials or compliance concerns. Coders should routinely review the latest updates to the ICD-10-CM official guidelines to stay informed about changes in classification and available codes.
To apply NEC codes correctly, it's important to recognize the types of situations where their use is appropriate. The following examples highlight common scenarios where selecting an NEC code supports accurate and compliant documentation.
Appropriate Scenarios for NEC Code Usage
NEC codes are typically used in situations where:
●
The provider documents a rare or
emerging condition that has not yet been assigned a specific code.
●
A subcategory exists for a general
condition, but none of the listed subcodes reflect the diagnosis described.
● A procedure or complication is documented with specificity, but the system lacks a direct code for it.
For instance, if a provider documents a newly observed variation of a known skin disorder, and no precise code is available under that category, a coder may choose an NEC option to reflect that level of detail. This practice ensures compliance, whether documenting routine conditions or rare medical practice findings that don't yet have full listings.
Documentation Must Support NEC Use
One of the most important rules for using NEC codes is that the provider's documentation must be thorough and clear. Coders cannot assume a diagnosis is specific, they must see it written explicitly in the medical record. Without proper documentation, using NEC is not only inappropriate but may result in inaccurate records and potential billing errors. In high-risk areas like Medicaid Services coding or healthcare services reimbursement, proper NEC use is especially critical.
This reinforces the importance of provider-coder collaboration. If documentation is incomplete or unclear, coders should reach out for clarification before assigning an NEC code.
Encouraging strong documentation habits can reduce the reliance on NEC and improve overall coding accuracy.
When NEC Is the Only Valid Option
NEC is not just a fallback in many cases, it is the only valid option. This typically happens when all other codes are ruled out due to specificity. Coders should carefully review the "includes" and "excludes" notes within the ICD-10-CM manual to confirm that no other more appropriate code exists.
If the diagnosis is clearly documented and does not match any of the existing subcategories, NEC provides a compliant, accurate, and justifiable coding solution.
Examples of NEC Codes in Action
Understanding how NEC codes are applied in real-world scenarios can help clarify when and why they should be used. These examples highlight cases where a provider documented a condition with specificity, but no exact ICD-10-CM code was available. They also show how NEC differs from unspecified codes that might be used if the documentation were less detailed.
Example 1: Focal Epilepsy with Unusual Presentation
A neurologist documents a diagnosis of "focal epilepsy with auditory hallucinations," a specific and rare manifestation of seizure activity. Upon reviewing the ICD-10-CM manual, the coder finds no subcategory under G40 (Epilepsy and recurrent seizures) that matches this particular presentation. Because the provider has clearly documented the condition, but no code exists to reflect that level of specificity, the coder selects G40.89 - Other seizures, which is an NEC code within the epilepsy category.
Why NEC was appropriate: The documentation was clear and detailed, but the classification system lacked a precise match.
If documentation were vague: If the provider had only written "seizures" without detail, the coder might have had to select G40.909 - Epilepsy, unspecified, not intractable, without status epilepticus, which is an NOS code and reflects insufficient detail.
Example 2: Postoperative Pain in a Rare Surgical Site
A patient experiences significant postoperative pain following a complex reconstructive ear surgery. The provider documents the pain specifically as "postoperative neuropathic pain in the external ear canal." However, ICD-10-CM does not provide a distinct code for this exact location. The coder uses G89.28 - Other chronic postoperative pain, which is an NEC code indicating a well-defined diagnosis not captured elsewhere.
Why NEC was appropriate: The diagnosis was specific, but ICD-10 lacked a more targeted code for pain in the external ear canal after surgery.
If documentation were vague: If the provider had simply documented "postoperative pain" without specifying the location or type, the coder might have used G89.29 - Other pain, an NOS code that reflects non-specific documentation.
Example 3: Adverse Effect of a New, Unlisted Medication
A patient develops a documented adverse reaction to a newly released antiviral medication. The provider writes "adverse effect of [specific drug name]" and includes the nature of the reaction in detail. The drug is not yet listed in the ICD-10-CM tables. The coder selects T50.99XA - Adverse effect of other drugs, medicaments and biological substances, initial encounter, an NEC code used when no specific drug-related code is available.
- Why NEC was appropriate: The adverse effect was clearly documented and linked to a named drug, but no classification code yet exists for that specific substance.
- If documentation were vague: If the provider had not specified which drug caused the reaction or described the reaction itself, the coder might have had to choose an unspecified adverse effect code, which would not meet documentation standards.
These examples illustrate how NEC coding allows providers and coders to maintain a high level of diagnostic accuracy even when the classification system does not yet provide a perfect fit.
By comparing NEC with what would be used in the case of vague documentation, it becomes clear why specificity is always the goal.
Best Practices for NEC Code Accuracy
Using the NEC code correctly requires more than just following guidelines. It involves careful attention to documentation, consistent collaboration between coders and providers, and a clear understanding of when NEC is truly appropriate. Medical billers and coders must work together to ensure that standardized codes are applied appropriately to reflect the complexity of medical procedures and services.
These best practices help ensure that NEC codes are applied only when justified and that medical records remain accurate and compliant.
1. Focus on Specificity in Documentation
The most important factor in determining whether an NEC code is appropriate is the level of detail in the provider's documentation. Coders must be able to identify a clearly described diagnosis that cannot be matched to any specific ICD-10-CM code.
If the diagnosis is vague or lacks supporting clinical information, NEC should not be used.
Encouraging providers to document the nature, location, and cause of a condition when possible helps reduce unnecessary use of general codes and supports proper NEC assignment.
Specificity benefits not only coding but also the accuracy of clinical records, billing, and quality reporting.
2. Strengthen Coder-Provider Collaboration
Open communication between coders and providers plays a key role in NEC code accuracy. Coders should feel empowered to query providers when documentation is unclear or when they believe more detail is needed to determine whether NEC is appropriate.
This collaboration should not be viewed as a correction, but rather as a partnership to ensure the patient record reflects the most accurate clinical picture.
Over time, consistent feedback from coders can also help providers improve the specificity of their documentation habits.
3. Avoid Overusing NEC Codes
While NEC is a legitimate part of the ICD-10-CM system, overuse can be a red flag during audits or reviews. Relying too heavily on NEC may suggest that coders are not fully reviewing available codes or that providers are not offering adequate detail. Coders should always search thoroughly within the classification system before defaulting to an NEC option.
Routine audits of code usage can help organizations monitor patterns and address any areas where NEC might be incorrectly or excessively applied.
4. Use NEC Only When No Exact Code Exists
The defining rule for using an NEC code is simple: there must be no existing ICD-10-CM code that matches the documented diagnosis. If a more specific code is available, it must be used, even if NEC appears to be a reasonable alternative.
Coders should take time to read all relevant notes in the codebook, including "includes," "excludes," and "code also" instructions that may clarify the best choice.
By applying NEC codes only when absolutely necessary, healthcare organizations can ensure compliance, avoid claim denials, and maintain the quality of their medical records.
The Impact of NEC Coding on Compliance and Data Quality
Accurate use of the NEC code plays a critical role in ensuring medical records are complete, claims are processed correctly, and healthcare organizations stay compliant.
NEC coding is not just about selecting a default option. It reflects a coder's ability to match highly specific provider documentation with the best available classification when no exact code exists, whether coding complex hospitalizations, code black emergencies, or routine outpatient care.
Why Proper NEC Code Usage Matters
When used correctly, NEC codes help maintain the integrity of documentation, especially in situations where ICD-10-CM has not yet created a code for a detailed diagnosis. This precision supports medical necessity, improves claim accuracy, and reduces the risk of denials or audits.
NEC codes also impact quality reporting by capturing nuanced clinical conditions that may otherwise be overlooked. In value-based care environments, that level of detail contributes to clearer performance data and more accurate health outcomes, even during high-priority events like code black scenarios where rapid, detailed documentation is critical.
To ensure continued accuracy, coders should stay current with the latest ICD-10-CM updates and work collaboratively with providers to support high-quality documentation. By applying NEC codes only when justified, and supported by specific documentation, healthcare teams can improve compliance, reduce coding errors, and deliver more complete data for both patient care and system-wide analysis.
At Healthcare Compliance Pros, we know that proper use of NEC codes is critical for maintaining complete, accurate, and compliant medical records. Coding errors, even small ones, can lead to claim denials, audit risks, and gaps in quality reporting. That's why we offer tailored compliance programs, coding education, auditing support, and real-time guidance to help healthcare organizations stay current with evolving standards like ICD-10-CM updates and standardized coding systems.
If your team needs help improving documentation practices, strengthening coding accuracy, or preparing for audits, we're here to help. Contact Healthcare Compliance Pros today to learn how our solutions can minimize risk, optimize claims, and support stronger outcomes across your organization, all while helping health care professionals and medical coders meet the highest documentation standards.